What is ICU Readmission? (that is, how is it formally defined and measured?)
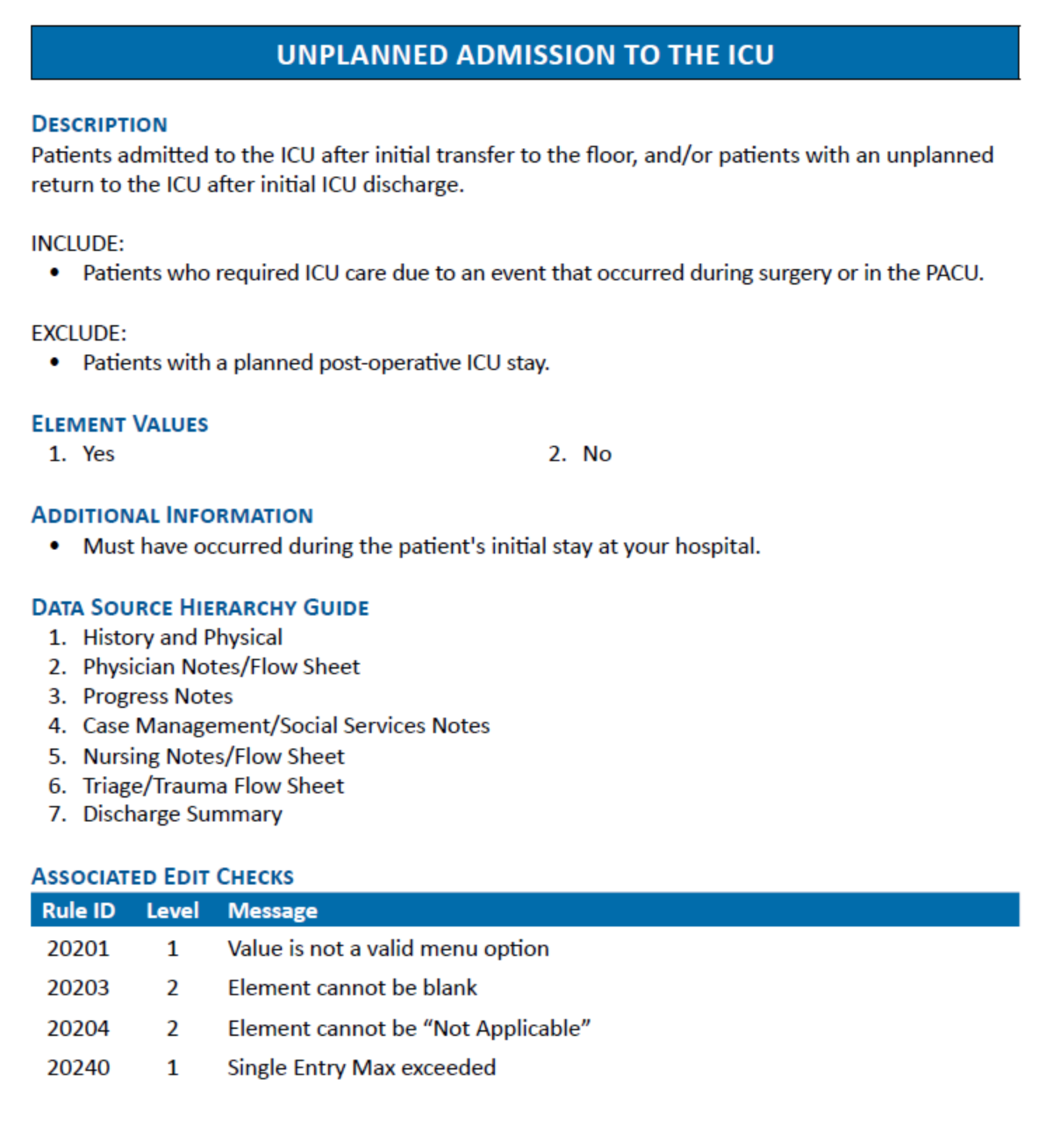
From Cincinnati: It doesn’t have to be a return to ICU - thus a broader term is “Unplanned Admissions to ICU”. We look at the ADT/Event Management Screens then review notes as to why the transfer to ICU occurred and collect as a complication. Society of Critical Care Medicine and TQIP define this as - a return to ICU within 48-72 hours, though some studies extend this to any time during the same hospital stay - ACS NTDS Data Dictionary screenshot:
How is ICU LoS calculated?
From Cincinnati: 1. For ICU we look at the ADT Events/Event Management in Epic and count the days from there, the patient must have a Level of Care as ICU to count as an ICU day. 2. Any partial day is counted as a full day per NTDS/TQIP. 3. For unplanned admissions to ICU (does not have to be a return to ICU, NTDS Data Dictionary screenshot below), we look at the ADT/Event Management Screens then review notes as to why the transfer to ICU occurred and collect as a complication. 4. We still count those days as towards the total ICU LOS.
How is it tracked in the system?
At Cincinnati, seems like unplanned admission to ICU is not tracked in Epic but in registry (process documented above.) - Broader health systems show manual chart review is still common. - registries like TQIP (Trauma Quality Improvement Framework) or NTDS (National Trauma Data Standard) are two major frameworks used by trauma centers to collect, standardize and analyze trauma-related patient data - some systems are moving toward EHR alerts based on deterioration indicators - Source: Cincinnati internal documentation; NTDS Unplanned ICU Admission Field Description (2023) - Source: Hauck et al., J Intensive Care Med, 2017; ACS Trauma Quality Programs Annual Report
Why is this a problem?
Manual tracking is labor intensive an inconsistent. Staff must manually review notes and ADT data, leading to missed or delayed identification. - w/out real-time alerts, clinical teams may miss early signs of deterioration. - ICU readmission is associated with up to 3x higher mortality and longer total LoS. - increases overall hospitalization cost (ICU stays are most expensive) - hospitals are benchmarked on ICU readmission as a marker of care coordination OTHER REASONS, NUMBERED AND BULLETED 1. Reactive, not predictive - EHRs track readmission but don’t necessarily predict them - clinicians often only see risk after the fact - too late to intervene 2. Data Silos - while some EHRs collect a lot of data, different departments (ICU, general ward, ED) may not share insights in real-time - disconnected workflows mean warning signs (ex. deteriorating vitals) are missed or buried in notes 3. Manual analysis bottlenecks - quality teams run retrospective reports monthly/weekly - by the time a high readmission rate is spotted, patterns are already entrenched 4. Limited real-time stratification - real-time, bedside decision support is limited Source: PMCAHA Journals
Do you have any process (or tool) in place currently to address this?
May centers use a registry-based tracking tool (ex. TQIP or local trauma registries) which collects complication data retrospectively.
If there is a process (or tool) in place currently, why is it not effective (or as effective as you’d like it to be)?
However, it is often ineffective because: - It does not enable real-time intervention - it is not integrated into clinician workflows - there are lags in data entry and processing - Source: ACS Trauma Registry Guidelines; Saria et al., NEJM AI in Healthcare Review, 2019
How do you expect to use an ICU Readmission predictive model?
Potential clinical and operational use cases include: - Real-time scoring in ED or post-op settings - Early warning systems that suggest ICU transfer before deterioration - Guidance for ICU discharge planning - ICU bed management optimization and resource allocation - AAFP
Apart from the ICU Readmission Rate, are there any other metrics (clinical, operational, financial) that may have similar underlying root causes and may be impacted with the use of a model like this?
Metrics that often correlate with ICU readmissions include: - Rapid Response Team (RRT) activations - Code Blue events after ICU discharge - Unexpected return to OR - Hospital-acquired complications (ex. pneumonia, sepsis) - 30-day hospital readmissions - ED boarding time before ICU transfer - Source: TQIP Reports; Wunsch et al., Crit Care Med, 2012 These issues often share upstream failures such as - early discharge - inadequate monitoring - poor transitions of care
Questions for internal discovery
Discovery Questions
How is ICU Readmission typically defined in the industry?
Most studies define ICU readmission as an unplanned return to ICU during the same hospitalization, with a focus on returns within 48-72 hours to isolate potentially preventable causes. Common predictors include: - age, comorbidities (the presence of 2 or more medical conditions), initial severity - discharge vitals and lab values - ventilation status - ICU LoS
Is it a big problem? (financial, clinical perspective)
Yes, ICU readmissions are a significant concern due to their association with increased mortality, longer hospital stays, and higher healthcare costs. They also serve as indicators of the quality of care and effectiveness of discharge planning. Wiley Online Library
How have health systems tried to solve it?
Health systems have implemented various strategies to reduce ICU readmissions, including: - developing ICU discharge checklists - establishing post-ICU follow-up programs - Implementing early warning systems like the Modified Early Warning Score (MEWS). - Integrating predictive analytics into EHRs. - Enhancing communication during care transitions. Medicina Intensiva These interventions aim to identify at-risk patients early and ensure appropriate post-ICU care.
What existing research is out there regarding an ICU Readmission predictive model?
Recent studies have explored the use of machine learning models to predict ICU readmissions. For example, a study developed a predictive model using Gradient Boosted Machines (GBM) and demonstrated its effectiveness in identifying patients at risk of readmission. PMC1PMC2 Another study employed a hybrid model combining BERTopic and Long Short-Term Memory (LSTM) networks to predict ICU readmissions, showing promising results. PMC3
Summary of existing work and research
Paper
Notes and Comments
Notes: - https://drive.google.com/file/d/1-cQrQw7Hnczzn1Yzjtxm1nweOwu9APdV/view?usp=drive_link - Very strong paper overall - Strong methods section - Good definition of outcome variable (“readmission) - Good detail on predictor variables - Uses GBM for the model Action items based on this paper - How does our definition of ‘readmission’ align with theirs? - How was the dataset / target value (readmission) derived? - How does our data set compare with the variables that they used? - Compare dataset in terms of sample size and positive flag rate - What is the lookback window of the different features? - What is the evaluation method? - Retrospectively on past data - Possibly future implementation - Are we missing anything that we should be adding?